It is well known that breech presentation for many women represents a great frustration, often feeling trapped after being offered a caesarean section as the only and "best" option for the birth of their child.
Fewer and fewer women have the opportunity to deliver their babies physiologically if they are breech, and often at unknown risks, as fewer and fewer obstetricians have sufficient knowledge and the desired skills to attend such births (Banks, 1998).
Midwives are well aware of our limits and we never plan to deliver a breech birth at home, it is not part of our remit (ICM, 2017; WHO, 1997), although it is our duty to be trained to deliver a breech birth in an emergency (Ministry of Health and Social Policy, 2009; ICM 2013; Keighley, 2009). However, we have a duty to offer women evidence-based options.

Is a breech vaginal birth safe?
Since 2017, it can now be said that breech vaginal birth is safe, as long as there is verticality and absolute freedom of movement on the part of the mother.
This type of birth (vs. breech birth with the mother lying down) is associated with a faster birth phase, reduction in the number of manoeuvres required, reduction in maternal and neonatal injuries and reduction in the number of caesarean deliveries (Louwen et al, 2017) and the same if the mother is on all fours (Bogner, 2014).
Vaginal breech birth does not pose an increased risk to child health in terms of long-term development and educational attainment compared to caesarean birth (Sun Bin, 2016).
Despite this, there are few trained and skilled professionals who know how to deliver a breech birth with skill.
It is often only accessed if the woman agrees to have epidural analgesia, which clearly increases the risk of delivery (Louwen et al, 2017).
I have often observed the courage, determination and willpower of many women who desire a physiological birth but feel trapped in the face of an unavoidable caesarean section and therefore try everything in their power to turn breech babies to a cephalic (head down) presentation.

Although External Cephalic Version (ECV) is a fairly safe, effective (50%) manoeuvre (Impley et al, 2017; RCOG, 2017; Hofmeyer et al, 2015; Hutton et al, 2015), and valid for many women; some feel it is too invasive for them and want to try other options first.
Thousands of years of Chinese medical history, and now also diverse scientific evidence, support the use of moxibustion at certain points on the body to encourage the baby to turn on its own (Xun et al, 2009; Van den Berg et al, 2008; Vas et al, 2008; Coyle et al, 2005) with positive results of approximately 50%. The possibility of assisting breech babies to turn through postures and/or exercises has also been studied, but the results are inconclusive (Hofmeyr and Kulier, 2012).
However, through deep body awareness work, the results I have observed so far combining moxibustion with a short and simple series of 3 exercises are 85% of success with a maximum of 10 days of treatment (Sàrries Zgonc, 2011). The mother only has to learn together with me how to do the exercises correctly and how to apply the moxibustion and she will be the one to do the treatment daily at the time of the day when she is calmer.
I usually work with mothers when they have reached 36 weeks of pregnancy to give the baby the possibility to turn on its own.
I would never work before, unless the mother asked me to, as I like to respect the baby's needs and rhythms, not without taking into account the emotional needs of the mother which can also play an important role.

Buttocks and emotions
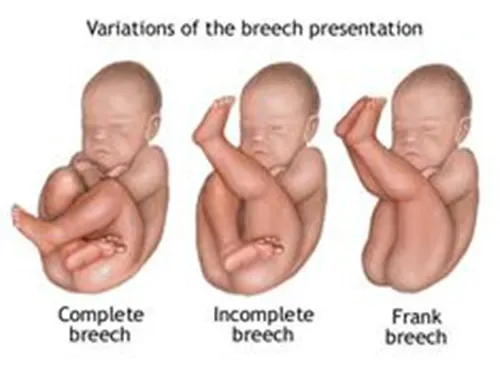
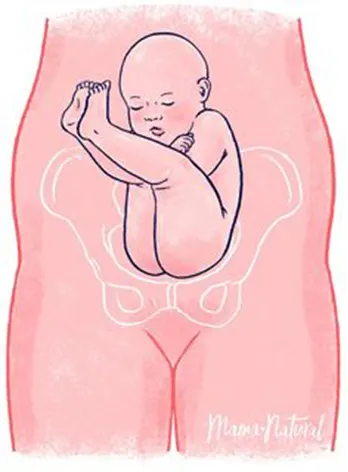
My experience has taught me that, apart from some physical predispositions, breech presentations are often a protective position that some intrauterine babies adopt when they perceive their mother's environment as dangerous and uncomfortable.
The head is very vulnerable, the skull protects the most precious part of the highly developed human body after thousands of years of evolution, and protecting it from danger is part of our instinct.
In fact, fearful children, in dangerous situations, adopt a position almost identical to that of intrauterine infants who present with their buttocks flexed, with their heads tucked between their knees and under their arms.
We all always instinctively protect our heads in dangerous situations.
After doing everything in our power to try to get babies to turn, they do not always turn easily into the cephalic position.
Occasionally, babies who had turned spontaneously, return to sitting on their buttocks.
I have noticed over time that some babies turn on their own when their mothers stop working or deal with a stressful situation in their environment.
Some mothers face conflicting feelings about their partners' reactions or the way they relate to them during pregnancy, or about important factors in their lives that concern them.
Simply allowing women to express their feelings almost always helps them to find a solution to some situations.
Often the babies of women who finally pay enough attention to their child turn spontaneously without any help.

Buttocks and hormones
The influences of the prenatal environment on endocrine function, and consequently on placental function, have been tested by studying maternal responses to stress, causing cardiovascular and endocrine changes in the mother, and increasing the amount of Adenocorticotropin, Catecholamines and Glucocorticoids (stress hormones) in the blood.
Kapoor et al (2006) suggest that increased levels of Glucocorticoids may trigger placental production of Corticotropin Releasing Hormone, activating the Hypothalamic-Pituitary-Adrenal axis, with increased production of Catecholamines, which may reduce the size of the placental lumen with a consequent reduction in blood supply to the intrauterine infant.
This, in turn, may further increase the activity of the Hypothalamic-Pituitary-Adrenal axis or put the fetal sympathetic nervous system on alert.
Every human being under stress will respond with the sympathetic nervous system, increasing blood pressure and pulse, blood clotting, activating suppression of pain sensitivity, redistributing blood from the gut to the limbs and brain (for internal protection) and releasing fat as a quick source of energy (Lundberg, 2005) to "run away from danger" as suggested by Üvnas-Moberg (2009).... or to hide.
We know that intrauterine babies often excrete meconium, especially when breech, simply because there is less blood supply to the intestines, along with a relaxation of the anal sphincter, as a protective response of the sympathetic nervous system to stress.
Üvnas-Moberg and Petersson (2006, 2005) emphasise that oxytocin increases and enhances our social behaviour, and thus emphasise how humans tend to isolate or become less sociable when under stressful situations.
Is the breech baby hiding or being less sociable because of fear of the unknown or because of perceived danger physiologically through hormones crossing the placenta?
We already know that the intrauterine baby can be very interactive and reactive to familiar voices, music, touch (Verny, 1982).
Why shouldn't it be interactive and reactive to unpleasant situations and sensations?
Given the historical moment we are living in today, caring only for women's security and satisfaction is not enough.
Women are spoilt for choice. But looking at the importance of oxytocin (or its absence) in health and social behaviour, we should ask ourselves about its importance for the survival of human beings and our society, especially during birth.
We should ask ourselves what Odent (2010) has already asked many times: "Can civilisation survive the caesarean?
Any midwife can easily state that her job is to care for the mother and baby to ensure their safety and satisfaction.
The treatment I offer to women (Sàrries Zgonc, 2011) provides both.
On the one hand, it gives the intrauterine babies the possibility to turn without being forced, only with stimulation through uterine relaxation and toning. On the other hand, it helps mothers to regain the possibility to give birth to their babies themselves.